Association of Aortic Knob Calcification with Intracranial Stenosis in Ischemic Stroke Patients
Article information
Abstract
Background and Purpose
Aortic knob calcification (AC) is associated with increased risks of cardiovascular and cerebrovascular events. We evaluated the clinical importance of AC in ischemic stroke patients with intracranial (IC) stenosis using simple, non-invasive and routine chest radiography.
Methods
The presence of AC was assessed in a chest posteroanterior view in 307 acute ischemic stroke patients admitted from May 2009 to April 2010, and who underwent magnetic resonance angiography or distal subtraction angiography. The association of AC with IC stenosis was analyzed.
Results
Patient age (68.3±8.7 vs. 65.9±8.27 years, P=0.04), and the prevalence of IC stenosis (70.7 vs. 41.3%, P<0.01) were higher in patients with AC than in patients without calcification. After adjusting for age, gender and vascular risk factors, logistic regression analysis showed that AC (Odds ratio, 3.54; 95% confidence interval, 1.90 to 6.61, P<0.01) and age (Odds ratio, 1.79; 95% confidence interval, 1.01 to 3.19; P=0.04) were independent factors affecting IC stenosis.
Conclusions
AC appears to be a reliable predictor for IC stenosis, an important mechanism of ischemic stroke.
Introduction
Calcium deposits in the arterial bed may indicate the extent of atherosclerotic lesions and aortic knob calcification (AC) is associated with increased risks of cardiovascular and cerebrovascular events.1-5 AC is also associated with coronary artery calcification or carotid atherosclerosis, and might have predictive and prognostic value for coronary artery disease.1,6,7 In addition, several reports have shown that aortic atherosclerotic disease or AC is related to ischemic stroke.4,8,9 But its clinical significance for ischemic stroke patients with intracranial (IC) stenosis, one of the major mechanisms of ischemic stroke, remains unclear.
Although thoracic computed tomography (CT) or digital subtraction angiograms are reliable in detecting aortic calcification,1,10 these imaging modalities are not routinely used. In this study, we evaluated the clinical importance of AC in ischemic stroke patients with intracranial stenosis by using simple, non-invasive routine chest radiography.
Methods
We studied 307 acute ischemic stroke patients within 7 days of onset, who were admitted to our department from May 2009 to April 2010, and who underwent magnetic resonance angiography or distal subtraction angiography. The patients were interviewed to collect information on the risk factors of ischemic stroke based on personal history of smoking, consumption of alcohol, diabetes mellitus, hypertension, family history and past history of stroke before entering the study. We excluded subjects if their chest X-rays were not properly centered, if they had any deviation of the trachea or shift of the mediastinum or if they had any known disease in the aorta, such as aortitis. We also excluded patients who had cerebrovascular events related to trauma, medical instrumentation, severe concomitant kidney (serum creatinine≥2.0 mg/dL) or liver disease, autoimmune disease, cerebral vaculitis or embolism from implants, such as an artificial heart valves or atrial fibrillation. Samples were collected from venous blood after a 12-hour overnight fast, and lipid profiles and standard blood tests were performed on admission.
All patients had chest radiography in the posteroanterior (PA) view. We examined the presence of calcification in the aortic knob (Figure 1A). Based on the findings of the cerebral angiogram, each segment of the carotid and vertebrobasilar arterial systems were classified as normal, stenosis or occlusion. These classifications were based on a neuroradiologist's report and a consensus by stroke specialists at a weekly stroke conference. The existence of any degree of stenotic lesion was interpreted as potential stenosis (Figure 1B).
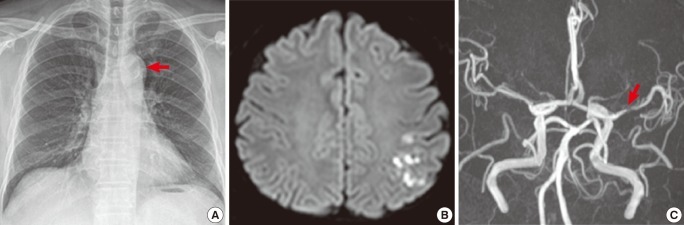
A 67-year-old man presenting with right hemiparesis with dysarthria (NIHSS 3 points). (A) Chest X-ray shows aortic knob calcification. (B and C) Diffusion-weighted image of magnetic resonance (MR) imaging (B) and MR angiography (C) of brain show a high signal intensity in the left MCA area with left MCA stenosis.
Data are presented as mean±standard deviation. Statistical analyses were done using SPSS® Ver.11.5 for Windows. Discrete variables were analyzed by the independent t-test and χ2 test. Spearman's correlation was used to examine the relationship between the aortic knob width and other risk factors. Logistic regression analysis was conducted to determine the factors related to intracranial atherosclerosis. Statistical significance was considered at P<0.05.
Results
Demographic characteristics of the study patients and risk factor profiles are shown in Table 1. The mean age of patients was 66.7±8.43 years and there were 191 male patients (62.2%). Among the 307 patients, there was stenosis in IC arteries in 151 patients (49.1%), in EC arteries in 68 patients (22.1%) and in both IC and EC arteries in 57 patients (18.5%).
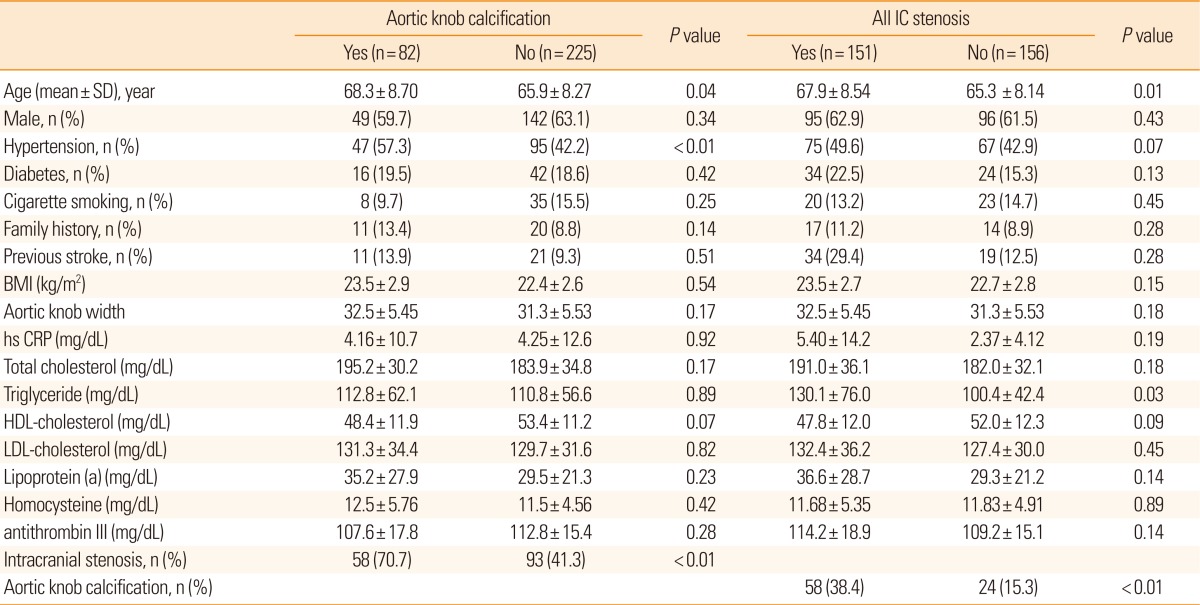
Clinical characteristics and laboratory findings of the study group
AC was present in 82 patients (26.7%) of the chest PA view. AC was observed more commonly in elderly patients and in patients with hypertension. There was no significant difference between the patients with or without AC in terms of diabetes, family history, smoking, aortic knob width and other risk factors, such as lipid profile, homocystein and high-sensitivity C-reactive protein levels. AC was observed in 58 (38.4%) patients with IC stenosis, 17 (25.0%) patients with EC stenosis and 17 (29.8%) patients with both stenosis of both the IC and EC arteries. Patients with AC had IC stenosis or IC+EC stenosis more frequently than those without calcification (P<0.01 and P=0.01, respectively). Unlike the patients with IC stenosis or those with IC and EC stenosis, patients with only EC stenosis did not have significantly more frequent AC (25%) than those without stenosis (15.3%) (P=0.08) (Figure 2). For patients of all EC stenosis (EC stenosis and IC+EC stenosis), there was no significant relationship indicated between AC (P=0.671). Logistic regression analysis showed that age (>65 years; Odds ratio (OR), 1.79; 95% confidence interval (CI), 1.01 to 3.19; P=0.04) and AC (OR, 3.54; 95% CI, 1.90 to 6.61, P<0.01) were independent predictors for IC stenosis after adjusting for age, gender, vascular risk factors and AC (Table 2).
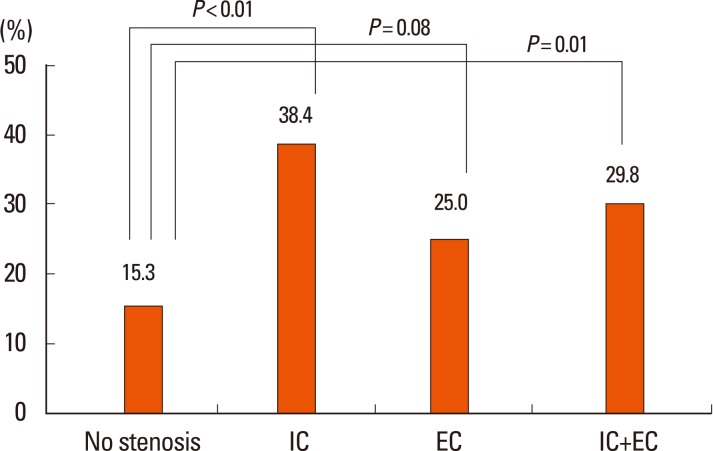
Frequency of aortic knob calcification in relation to intracranial stenosis (IC) or extracranial stenosis (EC).
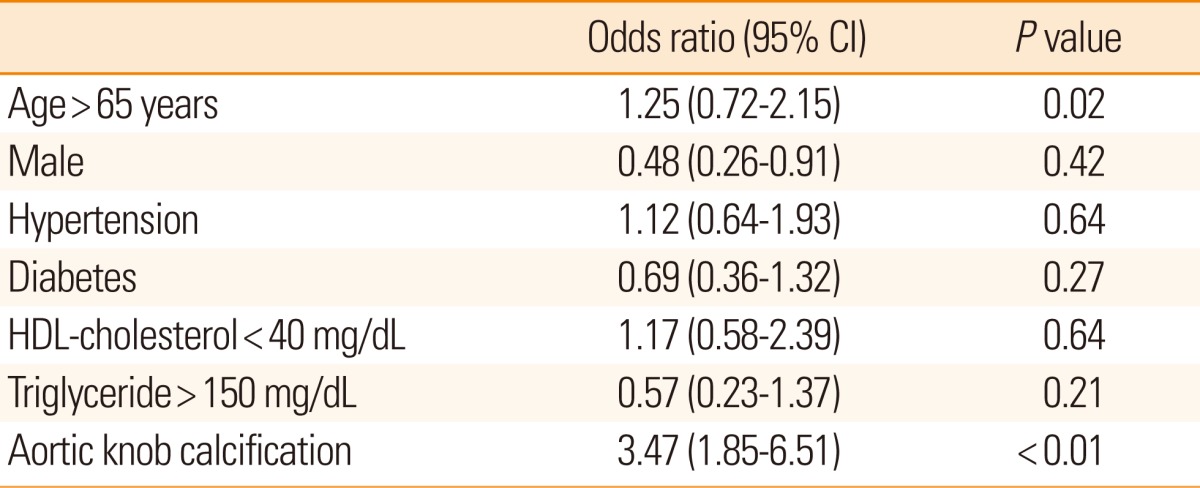
Logistic regression analysis of the clinical factors for IC stenosis
Discussion
The presence of AC in chest X-ray and age were correlated with IC stenosis in ischemic stroke patients. The detection of AC in chest X-ray may allow prediction of the presence of IC stenosis, which is an important mechanism in developing stroke. Chest radiography is a routine, non-invasive screening method and can reliably assess aortic calcification.7,11 Recently, interest has grown in arterial calcification in terms of risk factors and subsequent outcomes.
Arterial calcification is a complex, regulated process of biomineralization that resembles osteogenesis, which develops in the intima layer within atherosclerotic plaque, and which is a progressive feature of common atherosclerosis.2,12,13 Arterial calcification is associated with conventional atherogenic risk factors such as old age, diabetes, hypertension, cholesterol, or C-reactive protein and with an increased risk of cardiovascular and cerebrovascular diseases.2,14 This study also correlated AC with old age and hypertension, but had indicated a tendency of association with HDL-cholesterol, as the study population was comprised of ischemic stroke patients. Individuals with atherosclerotic disease occurring in one specific vascular bed have a higher risk of a clinical disease caused by atherosclerosis at another site.2,9,15 Thus, patients who suffer ischemic stroke or peripheral artery disease have a higher incidence of concomitant systemic artery disease, which may explain our results involving the simultaneous involvement of aorta and the IC artery, However, when we reanalyzed the association for predictors of EC stenosis after adjusting for age, sex and vascular risk factors, such as hypertension, diabetes mellitus and hyperlipidemia, a significant association was not found (OR, 0.56; 95% CI, 0.23 to 1.32; P=0.18), although we found a tendency of a correlation between AC and EC stenosis (P=0.08).
Our study has several limitations. The first is a selection bias because the study patients did not represent the general population. This is why AC was more common among the participants than in previous studies (2-3%),4 and AC was not correlated with EC athersosclerosis. Also, regardless of symptomatic or asymtomatic stenosis, we only included study patients of large artery atherosclerotic groups and small artery occlusion groups based on the Trial of ORG 10172 in Acute Stroke Treatment (TOAST) classification,16 in which AC showed no significance between the two groups (P=0.118). Secondly, we detected AC using only chest radiography. We could not confirm the presence of AC using other methods, such as electron-beam CT. We could not also include the other aortic atherosclerotic lesions, such as atheromas, protruding atheromas, or plaque, and thoracic segments of the aorta identified by transesophageal echocardiography. However, the present findings may well indicate the significance of aortic calcification by the use of just a simple chest x-ray, although the characteristics of the study patients and the diagnostic tools used in this study should be interpreted with caution.
In conclusion, our results suggest that AC is a reliable predictor for IC stenosis in ischemic stroke patients. An increase in the use of chest radiography as a screening or risk factor assessment tool may be justified.
Notes
The authors have no financial conflicts of interest.
This study was supported by the Wonkwang Institute of Clinical Medicine in 2011.