Automated Composition Analysis of Thrombus from Endovascular Treatment in Acute Ischemic Stroke Using Computer Vision
Article information

Dear Sir:
Histological analysis of thrombi acquired from endovascular thrombectomy for ischemic stroke provides an unprecedented understanding of thrombus formation in stroke [1]. Composition analysis is currently the mainstream of research for stroke thrombi, and immunohistochemistry (IHC) staining is frequently used [2,3]. Most studies have used general purpose software, including ImageJ and Photoshop (Adobe, San Jose, CA, USA) [4,5]. However, for composition analysis, these tools require manual drawing for area measurement, which is labor-intensive and prone to bias, and the results are irreproducible. This study aimed to develop an open-sourced software named Automated Region-of-interest based Image Analysis (ARIA) for automated composition analysis of IHC-stained thrombi.
This was a retrospective study using a nationwide multicenter prospective registry. The Specialized Multi-center Attributed Registry of sTroke–Clot (SMART-Clot) is a prospective registry that enrolls consecutive patients with acute ischemic stroke from 10 centers in Korea who underwent endovascular thrombectomy. Forty stained slides from 10 randomly selected patients were included in this study. Detailed methodology is described in the Supplementary Methods and Supplementary Figure 1. Screen recordings using both ARIA and traditional method for thrombus image analysis are presented in the Supplementary Video. The accuracy and time needed for analysis were compared between the traditional analysis method and ARIA. Four analysts with varying experiences measured the same 40 slides using both the traditional method and ARIA. External validation was performed for two datasets: (1) anti-CD42b IHC stained slides of stroke thrombi from a previously published study [6] and (2) an open dataset of IHC slides from breast tissue [7]. This study was approved by the Institutional Review Board of Yonsei University College of Medicine (Approval number: 4-2017-0426), and informed consent was obtained from each patient. ARIA is publicly available as an open-sourced project and can be installed in all major operating systems (https://github.com/jnheo-md/aria).
The median age of the patients included in this study was 71.5 years (interquartile range [IQR], 66.2 to 79.8) and six (60.0%) were male (Supplementary Table 1). The results obtained using ARIA by all analysts showed highly accurate results compared to the results from the professional analyst using the traditional method. The Spearman’s correlation coefficient of the stained ratio, defined as the stained area divided by the total area, ranged between 0.913 and 0.916 (all P<0.001) (Table 1). The Bland-Altman analysis showed 95% limits of agreement between 0.11 and 0.14 (Supplementary Figure 2). Agreement of the results from each analyst were significantly higher using ARIA than the traditional method for thrombus area (P=0.005), stained area (P<0.001), and stained ratio (P<0.001) (Table 2 and Supplementary Figure 3). The focused and total times needed for analysis were significantly shorter when ARIA was used than when the traditional method was used (Figure 1 and Supplementary Table 2). The median focused time needed while using ARIA was 7 seconds (IQR, 3.0 to 11.0), whereas the traditional method required a median of 231 seconds (IQR, 182.0 to 286.0; P<0.001). There was disagreement on one sample with homogeneous staining pattern due to differences in thresholding algorithm. There was high correlation, except for that sample with tissue factor staining, and significant analysis time difference between the two methods across each staining method and composition (Supplementary Tables 3 and 4, Supplementary Figure 4). External validation showed high correlation for both stroke thrombi and breast tissue (Spearman’s correlation coefficient 0.929 and 0.875 respectively, both P<0.001) with significant focused time reduction (median 7.0 seconds [IQR, 7.0 to 10.0] vs. 198.0 seconds [IQR, 184.0 to 313.0] in stroke thrombi; and 11.0 seconds [IQR, 8.0 to 13.0] vs. 185.0 seconds [IQR, 165.5 to 217.5] in breast tissue, both P<0.001).
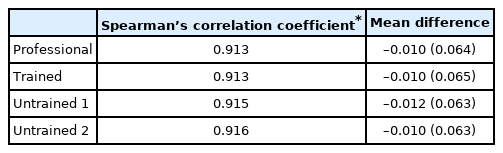
Comparison between stained ratio of each analyst using ARIA and those of the professional analyst using the traditional method

Differences between analysts for ARIA and traditional method

Comparison of (A) focused time and (B) total time needed for analysis using Automated Region-of-interest based Image Analysis (ARIA) and traditional methodology
This study validated a custom-built software named ARIA developed with computer vision for automated stroke thrombus composition analysis. ARIA (1) was highly accurate; (2) provided consistent results even for analysts without previous experience; and (3) was 30 times faster than the traditional method. Additionally, ARIA produced the same results when the input image and analysis parameters were equal, which is impossible using traditional methods.
Traditional method of composition analysis requires manual demarcation of the thrombus border, which is strenuous and inevitably introduces potential error due to inconsistencies in freehand drawing. ARIA mainly uses the Canny Edge Detection algorithm to replace freehand drawing, which is a widely used technique [8]. Additionally, slide image processing and automatic thresholding have been used in ARIA to reduce unnecessarily burden on the researchers [9,10]. Furthermore, this study demonstrated that the four analysts with varying experiences produced more consistent results when they used ARIA. Considering that the reproducibility and consistency between analysts are critical factors for a research methodology, ARIA has advantages for thrombus analysis over traditional methodologies.
This study has several limitations. The number of samples included in this study was small and originated form a single laboratory. There is no gold standard in measuring the composition of thrombi and the assessment of the accuracy of the novel software is limited. The expert’s analysis result using traditional method does not necessarily represent the true composition of the thrombus. As seen in one sample with exceptional disagreement between methods, thresholding algorithm may have great effect on the results, especially in images with homogeneous texture.
In conclusion, ARIA may be used as an efficient and accurate tool that provides reproducible results in thrombus analysis.
Supplementary materials
Supplementary materials related to this article can be found online at https://doi.org/10.5853/jos.2022.02054.
Characteristics of the patients included in the study
Time needed for analysis using ARIA and traditional methodology for each analyst
Comparison of results grouped by dominant component of the thrombus of each patient
Comparison of analyst results grouped by stained antibody
Imaging analysis process performed by Automated Region-of-interest based Image Analysis (ARIA). IHC, immunohistochemistry; CSV, comma separated value.
Bland-Altman plots of stained ratio results from each analyst using Automated Region-of-interest based Image Analysis (ARIA) compared to those of the professional analyst using the traditional method: (A) the professional analyst, (B) trained analyst, (C) untrained analyst 1, and (D) untrained analyst 2. SD, standard deviation.
Scatter plot showing distribution of the result differences between analysts of (A) stained ratio, (B) total thrombus area, and (C) stained area for the same slide image using Automated Region-of-interest based Image Analysis (ARIA) and traditional methodology. Differences from all possible combination of two analysts were plotted.
Scatter plot showing distribution of the result differences between analysts of (A) anti-CD42b, (B) anti-glycophorin A, (C) anti-fibrinogen, and (D) anti-tissue factor-stained slides using Automated Region-of-interest based Image Analysis (ARIA) and traditional methodology. Differences from all possible combination of two analysts were plotted.
Notes
Disclosure
The authors have no financial conflicts of interest.
Acknowledgements
This research was supported by a grant of Patient-Centered Clinical Research Coordinating Center (PACEN) funded by the Ministry of Health & Welfare, Republic of Korea (grant number: HC19C0028) and the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT) (grant number : 2022R1I1A1A01063439).
We would like to thank the students (S.Y. Kang and N.Y. Baik) who participated in this study.