Dear Sir:
Multiple multicenter randomized clinical trials have established mechanical thrombectomy (MT) as the standard of care (SOC) for large vessel occlusion (LVO) acute ischemic strokes (AIS) [1]. It is also established quite definitely that in the early thrombectomy window (0 to 6 hours), the neurological functional outcome is highly time-sensitive and designing workflow to minimize delays of even few minutes is critical [2]. Currently, more than 1 million cardiac catheterization (CC) procedures are performed annually in the United States. The reported incidence of acute stroke during CC in the literature ranges from 0.1% to 0.6% [3] and if a LVO stroke, can result in lifelong disability. Use of intravenous recombinant tissue plasminogen activator (IV-rtPA) therapy for AIS during CC is not well established with concern for relatively higher risk of bleeding due to procedural anticoagulation. With arterial access already in place, an immediate “direct” cerebral digital subtraction angiogram (cDSA) can expedite a definitive diagnosis of LVO allowing rapid MT in such patients. Finding a LVO on immediate cDSA in a patient with acute stroke syndrome during CC makes the possibility of concurrent intracerebral hemorrhage (ICH) highly unlikely as a cause of the syndrome. A conventional head computed tomography (CT) necessitates moving the patient from the CC laboratory table to CT and then to neuro-angiography suite which adds significant delay to reperfusion benefit.
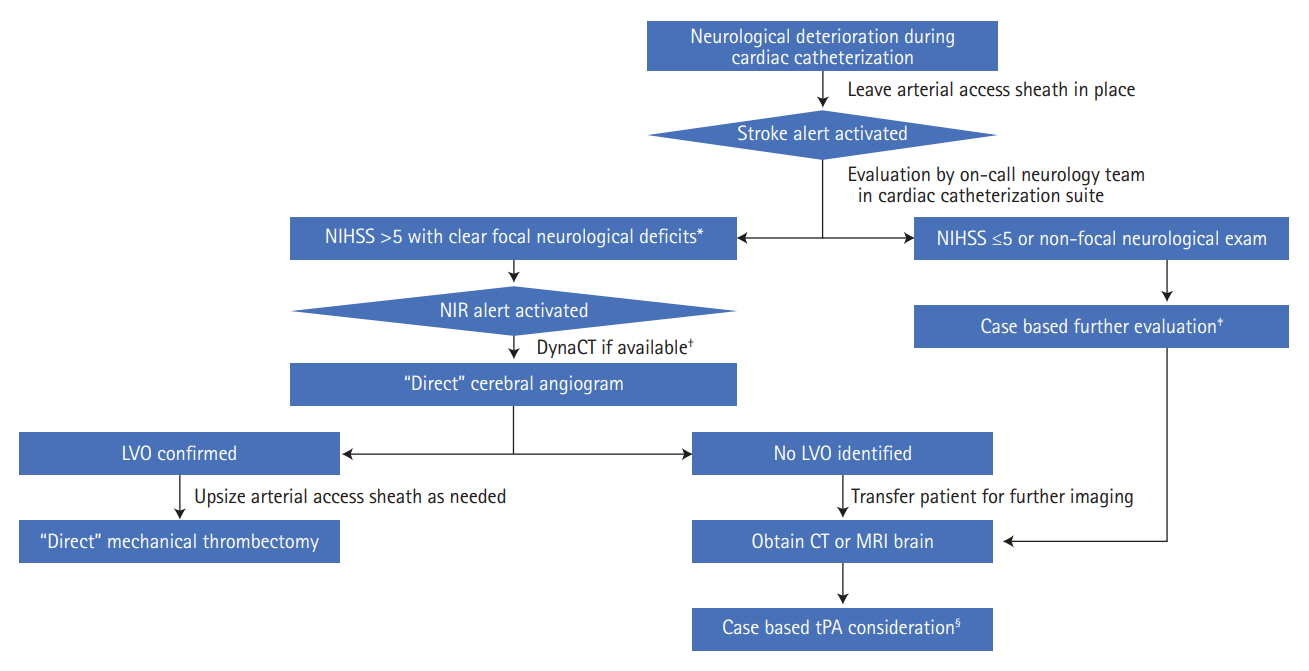
We hypothesized that a novel triage strategy of “direct” cDSA, bypassing conventional head CT, followed by MT in patients who suffered a LVO AIS during CC procedures is safe and would keep the onset-to-reperfusion times short. “Direct” is defined as performing cDSA for MT in the same single-plane CC suite foregoing conventional CT to rule out ICH. In this case series we report two large tertiary-care comprehensive stroke centers experience with this management strategy, which was agreed upon by both cardiology and neuro-endovascular teams. All direct-cDSA and MT procedures were performed by Endovascular Surgical Neuroradiology fellowship-trained neuro-interventionalists. Figure 1 highlights our institutional workflow algorithm for direct-cDSA.
Four consecutive cases were included in this case series from January 2016 to June 2017, where the acute focal neurological syndrome was identified while patients were still in the CC suite and had the arterial sheath in place. Table 1 details the baseline characteristics and covariates of patients included in this case series. All patients identified were undergoing emergent CC, three for NSTEMI and one for unstable angina. A CT brain was obtained within 24-hour post-MT to evaluate for any hemorrhagic transformation (HT) of the infarcted cerebral tissue. LVO was confirmed in three out of four patients who subsequently underwent successful MT (Figure 2). One patient had patent vessels on direct-cDSA with rapid improvement in symptoms suggesting spontaneous recanalization or non-LVO stroke. Immediate head CT obtained in this patient did not show an ICH, and IV-rtPA was not administered because symptoms spontaneously improved with return of National Institutes of Health Stroke Scale to 0. In aggregate, the mean times from the identification of neurological deficits to start of cDSA procedure, first pass and successful revascularization was 17, 43 and 54 minutes, respectively. In all cases, the same transfemoral arterial access (TFA) obtained by a cardiologist was utilized for initial cDSA with subsequent upsizing of the access sheath to 8 Fr as needed for MT. Anticoagulation with intravenous unfractionated heparin during CC procedures was used in three of four patients. IV-rtPA was not administered in any case. All CC procedures were performed under monitored anesthesia care, and none of the patients required conversion to general anesthesia for MT. Solitaire stent retriever with balloon guide catheter and standard endovascular stroke techniques were used for all MT procedures.
Since MT became SOC in 2015 and the outcomes were found to be highly time sensitive [1], a major focus is to devise time saving workflow strategies to maximize good outcomes. Our case series indicate that if a LVO is seen on cDSA in the vascular territory referable to the stroke syndrome occurring during CC, the need for a CT to rule out hemorrhage appears to be redundant. None of the patients in our series had a HT on subsequent CT brain indicating safety of our approach. There is anecdotal evidence documenting the safety of reversal of procedural anticoagulation with IV heparin with protamine followed by successful administration of IV-rtPA for AIS during CC [4]; but as there is no clear consensus on this approach we opted to forego the same.
In keeping with the trend of preferred increased use of trans-radial access for cardiovascular procedures, it is important to highlight the fact that successful MT can be performed using the same radial access which can be upsized to 6 Fr as needed, without the need for crossover to TFA [5]. Furthermore, the angiographic suites equipped with the newer flat-panel detector technology have the capability of obtaining a sufficient quality DynaCT (Siemens Medical Solutions, Erlangen, Germany), which can be used to rule out ICH [6] and if negative, would obviate the need to remove the patient from angiography table supporting our approach for direct-MT.
Our case series suggests that performing immediate direct cDSA followed by MT without conventional CT is feasible, safe and keeps the stroke onset-to-reperfusion times very short in patients with suspected LVO during CC procedures. Therefore, further and larger studies are needed to prove the use of this approach in routine clinical practice.