Robot-assisted Therapy in Stroke Rehabilitation
Article information
Abstract
Research into rehabilitation robotics has grown rapidly and the number of therapeutic rehabilitation robots has expanded dramatically during the last two decades. Robotic rehabilitation therapy can deliver high-dosage and high-intensity training, making it useful for patients with motor disorders caused by stroke or spinal cord disease. Robotic devices used for motor rehabilitation include end-effector and exoskeleton types; herein, we review the clinical use of both types. One application of robot-assisted therapy is improvement of gait function in patients with stroke. Both end-effector and the exoskeleton devices have proven to be effective complements to conventional physiotherapy in patients with subacute stroke, but there is no clear evidence that robotic gait training is superior to conventional physiotherapy in patients with chronic stroke or when delivered alone. In another application, upper limb motor function training in patients recovering from stroke, robot-assisted therapy was comparable or superior to conventional therapy in patients with subacute stroke. With end-effector devices, the intensity of therapy was the most important determinant of upper limb motor recovery. However, there is insufficient evidence for the use of exoskeleton devices for upper limb motor function in patients with stroke. For rehabilitation of hand motor function, either end-effector and exoskeleton devices showed similar or additive effects relative to conventional therapy in patients with chronic stroke. The present evidence supports the use of robot-assisted therapy for improving motor function in stroke patients as an additional therapeutic intervention in combination with the conventional rehabilitation therapies. Nevertheless, there will be substantial opportunities for technical development in near future.
Introduction
Stroke is a common, serious, and disabling health-care problem throughout the world.1 In particular, in Korea, which is very rapidly changing into an "Aging Society," the incidence of stroke has increased, albeit gradually, during the last few decades.2 On the other hand, the mortality rate from stroke has declined over time,2 resulting in an increased prevalence of stroke in Korea. Unfortunately, one third of stroke survivors achieve only a poor functional outcome five years after the onset of stroke.3 Therefore, stroke-related problems are a serious burden to both patients and their families.4 Although great advances have been made in acute stroke management, the majority of post-stroke care to reduce patients' dependency relies on rehabilitation treatments.
Neuroplasticity is the basic mechanism underlying improvement in functional outcome after stroke.5 Therefore, one important goal of rehabilitation of stroke patients is the effective use of neuroplasticity for functional recovery. Other principles of stroke rehabilitation are goal setting, high-intensity practice, multidisciplinary team care, and task-specific training.1 Therefore, high-dose intensive training6 and repetitive practice of specific functional tasks7 are important for recovery after stroke. These requirements make stroke rehabilitation a labor-intensive process.
Robotic technology has developed remarkably in recent years, with faster and more powerful computers and new computational approaches as well as greater sophistication of electro-mechanical components.8 This advancement in technology has made robotics available for rehabilitation intervention. A robot is defined as a re-programmable, multi-functional manipulator designed to move material, parts, or specialized devices through variable programmed motions to accomplish a task.9 The most important advantage of using robot technology in rehabilitation intervention is the ability to deliver high-dosage and high-intensity training.10 This property makes robotic therapy a promising novel technology for rehabilitation of patients with motor disorders caused by stroke or spinal cord disease. Research into rehabilitation robotics has been growing rapidly, and the number of therapeutic rehabilitation robots has increased dramatically during the last two decades.11
Rehabilitation robots can be divided into therapeutic and assistive robots. The purpose of assistive robots is compensation, whereas therapeutic robots provide task-specific training.12 In this manuscript, the authors will focus on the usefulness of therapeutic robots in patients with stroke. The types of robotic devices used for motor training are end-effector-type devices and exoskeleton-type devices (Figure 1).13 End-effector devices work by applying mechanical forces to the distal segments of limbs. End-effector type robots offer the advantage of easy set-up but suffer from limited control of the proximal joints of the limb, which could result in abnormal movement patterns. In contrast, exoskeleton-type robotic devices have robot axes aligned with the anatomical axes of the wearer. These robots provide direct control of individual joints, which can minimize abnormal posture or movement. Their construction is more complex and more expensive than that of the end-effector type. In this manuscript, the authors will summarize the recent research concerning both the end-effector and exoskeleton types of robot devices. We will also discuss the current status of robot-assisted therapy in stroke rehabilitation.
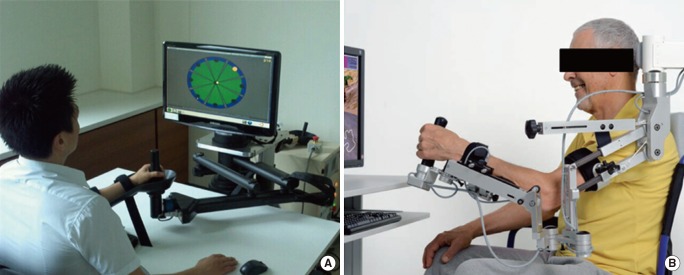
Examples of robotic devices for motor training (A) End-effector type (InMotion 2.0 Interactive Motion Technologies, Watertown, MA, USA), (B) Exoskeleton type (Armeo®, Hocoma, Switzerland).
Robot-assisted therapy for gait function
End-effector-type robotic devices
Seven randomized controlled trials that compared robot-assisted therapy that uses end-effector-type devices with conventional therapies for improving gait function after stroke were selected for review (Table 1).14-20

Robot-assisted therapy for gait function
Two studies conducted in patients with chronic stroke reported comparable effects on gait function between the robot-assisted therapy and conventional gait training.14,17 These results indicate that the robot-assisted therapy with end-effector-type devices cannot replace conventional therapy in patients with chronic stroke. However, the other five trials, which enrolled patients with subacute stroke, demonstrated that robot-assisted therapy in combination with conventional physiotherapy produced greater improvement in gait function than conventional gait training alone.15,16,18-20 This means that the addition of robot-assisted therapy with end-effector-type devices to conventional physiotherapy can be recommended for use in patients with subacute stroke.
Exoskeleton-type robot devices
Eight randomized controlled trials that investigated the use of robot-assisted therapy with exoskeleton devices for improvement of gait function in patients with stroke were selected for review (Table 1).21-28 Two studies from 2007 reported superior results from robot-assisted therapy with exoskeleton devices in comparison with conventional physiotherapy.24,26 Both trials recruited relatively small numbers of patients. The first was a pilot study in patients with subacute stroke.24 Then, in 2008, Hornby et al.23 performed a randomized controlled study comparing the effects of robot-assisted gait training that uses exoskeleton devices and manual facilitation that uses an assist-as-needed paradigm on gait function in patients with chronic stroke. Their results demonstrated that therapist-assisted training yields greater improvements in walking ability in ambulatory stroke survivors than does a similar dosage of robot-assisted training. Hidler et al.22 also investigated the usefulness of robot-assisted therapy in patients with subacute stroke in a multicenter randomized trial. They concluded that the diversity of conventional gait training interventions appeared to be more effective than robot-assisted gait training for improving walking ability. Therefore, these two reports agreed that at similar training intensities, conventional therapy is more effective than robot-assisted therapy with exoskeleton devices for recovery of gait function after stroke. However, other reports documented similar or superior effects of robot-assisted therapy in combination with conventional physiotherapy versus conventional therapy alone on gait recovery, especially in patients with subacute stroke.21,27 In 2009, a study by Schwartz et al.49 with a larger number of participants concluded that locomotor therapy by using robot devices in combination with regular physiotherapy produced promising effects on gait function in patients with subacute stroke in comparison with regular physiotherapy alone.27 Therefore, robot-assisted therapy with exoskeleton devices may not be able to replace conventional physiotherapy for improving gait function in patients with stroke but rather is recommended for use in combination with conventional physiotherapy, preferably in the subacute stage of stroke. However, there is insufficient research on the additional effect of robot-assisted therapy on gait function in the chronic stage of stroke.
Robot-assisted therapy for upper limb and hand motor function
End-effector-type robotic devices
Fourteen randomized controlled trials comparing robot-assisted therapy that use end-effector-type devices with conventional therapies for improvement of upper limb motor function after stroke were selected for review (Table 2).29-41 The meta-analysis in a 2012 Cochrane review demonstrated that robot-assisted arm training improved upper limb function (standardized mean difference 0.45; 95% confidence interval (CI), 0.20 to 0.69; P=0.0004).42 However, more detailed analysis is needed to develop guidelines for individual stroke rehabilitation. A study by Fasoli et al.32 comprising 56 patients with subacute stroke reported that patients who received conventional therapy alone showed little improvement, whereas patients who received robotic training plus conventional therapy continued to improve in the latter half of the inpatient rehabilitation period. This means that robot-assisted therapy is effective for improving upper limb motor function in patients with subacute stroke. A study by Lo et al.36 that recruited 127 chronic stroke patients reported that robot-assisted therapy and conventional therapy produced similar amounts of improvement after 12 weeks of treatment. However, after 36 weeks of therapy, the robot-assisted therapy achieved greater motor improvement than did conventional therapy. A study in patients with chronic stroke by Hsief et al.34 also found significantly greater improvement in upper limb motor function in the higher-intensity robot-assisted training group than in the control treatment group. In contrast, upper limb motor recovery did not differ significantly between the lower-intensity training group and the control group. These findings suggest that the intensity is the most important parameter of robot-assisted therapy for upper limb motor recovery in patients with chronic stroke.

Robot-assisted therapy for upper limb motor function
Nine of the 14 randomized controlled trials that examined robot-assisted therapy with end-effector-type devices assessed the influence of robot-assisted training on activities of daily living (ADL) in patients with stroke.29,30,32-35,38-41 These nine reports demonstrated that robot-assisted training yielded similar or better effects on ADL in comparison with conventional therapy. The 2012 Cochrane review meta-analysis demonstrated that robot-assisted arm training improved ADL performance (SMD, 0.43; 95% CI, 0.11 to 0.75; P=0.009).42 In addition, studies in patients with subacute stroke suggested that patients who received additional robotic therapy showed greater improvements in ADL.32,40 However, trials in patients with chronic stroke demonstrated no additional improvement in ADL over conventional therapy.34 In summary, robot-assisted therapy for upper limb motor function provides an additional effect on ADL function only in patients with subacute stroke. Further studies may be needed to draw a definite conclusion about the effect of robot-assisted training on ADL in patients with chronic stroke.
Three randomized controlled trials concerning hand motor function in patients with stroke were selected for review (Table 3).43-45 All three studies showed similar or superior effects of robot-assisted training in comparison with conventional therapy on hand motor function in patients with stroke. Hwang et al.45 demonstrated that robot-assisted therapy provided dose-dependent improvement in hand function. However, all three trials were single-center studies with relatively small numbers of participants, all in the chronic stage of stroke, and there was no randomized controlled trial that included subacute stroke patients as participants Furthermore, there was no assessment of ADL function after robot-assisted therapy for hand motor function. Therefore, these results suggest that robot-assisted therapy with end-effector devices may yield similar or greater improvement in hand motor function in patients with chronic stroke, but there is insufficient research to support an effect in patients with subacute stroke. Therefore, well-designed studies are needed to draw clear conclusions regarding the effect of robot-assisted therapy that use end-effector-type devices on improvement of the hand motor function of patients in both the subacute and chronic stages of stroke.
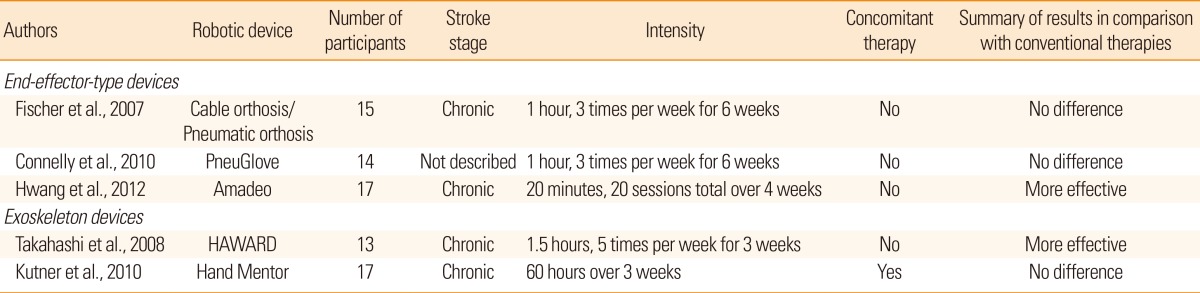
Robot-assisted therapy for hand motor function
Exoskeleton-type robot devices
Four randomized controlled trials of robot-assisted therapy with exoskeleton devices for improvement of upper limb motor function after stroke were selected for review (Table 2).46-49 All 4 trials were performed in patients in the chronic stage of stroke. Among them, one study reported a significantly better effect on spasticity in the robot-assisted therapy group than in the conventional therapy group.46 In contrast, ADL function improved more markedly in the conventional therapy group that received the same amount of treatment. The other three reports demonstrated no significant difference between robot-assisted therapy with exoskeleton devices and conventional therapies.47-49 In addition, there was no randomized controlled trial that investigated robot-assisted therapy with exoskeleton devices in patients with subacute stroke. Therefore, at this time there is insufficient evidence to draw a definite conclusion regarding the effect of robot-assisted therapy that uses exoskeleton devices on upper limb function in patients with stroke.
Two randomized controlled trials that examined robot-assisted therapy with exoskeleton devices for improving the hand motor function of patients with stroke were selected (Table 3).50,51 Both studies showed similar or better results on hand motor function in comparison with conventional therapy. However, neither trial recruited patients in the subacute stage of stroke or assessed the effect of robot-assisted therapy on ADL function. In summary, robot-assisted therapy that uses exoskeleton devices may provide similar or additional benefits for hand motor function in comparison with conventional therapy in patients with chronic stroke, but there is insufficient evidence regarding the effect of robot-assisted therapy with exoskeleton devices on the hand motor function of patients in the subacute stage of stroke.
Conclusions
Numerous recent studies have heralded the introduction of robotic devices into the field of stroke rehabilitation. Many reports have described the efficacy of robot-assisted therapy for improving motor and ambulatory function in patients with stroke. However, both ethical and methodological constraints hinder the design of double-blind randomized controlled studies of robot-assisted therapy in patients with stroke. Furthermore, there are only a few well-organized comprehensive reviews of robot-assisted therapy.13,42,52,53 Meta-analysis of robot-assisted therapy is very difficult because of the heterogeneity of the robotic devices and the participants' characteristics as well as the diversity of the study designs in the literature. Therefore, it is important to consider expert opinion as well as research data in order to draw the best conclusions. In this review, we made an effort to analyze the effects of different types of robotic devices on upper limb and hand motor function as well as gait function. In summary, the role of robot-assisted therapy in stroke rehabilitation is currently an adjunct to rather than a replacement for conventional rehabilitation therapy. Well-designed studies with large numbers of participants that demonstrate superior efficacy for motor recovery will be necessary to establish robot-assisted therapy as an integral part of stroke rehabilitation. Analysis of the economic impact as well as the functional benefits of robot-assisted therapy is also needed. Robot-assisted therapy for stroke rehabilitation is in a dynamic phase of development and has achieved remarkable advances. Ongoping improvement of the robotic technology may enhance the efficacy and reduce the cost of such devices. Such advances will elevate robot-assisted therapy to a standard therapeutic modality in stroke rehabilitation.
Notes
This article was supported by a KOSEF grant (M10644000022-06N4400-02210) funded by the Korean government.
The authors have no financial conflicts of interest.