Dear Sir:
Atrial fibrillation (AF) and patent foramen ovale (PFO) are potential causes of stroke [1-3]. When a patient has both AF and PFO, the risk of stroke/thromboembolism from one of these conditions may be affected by the other [4]. However, this issue has rarely been investigated.
AF is often accompanied by left atrial (LA)/LA appendage (LAA) thrombus and spontaneous echo contrast (SEC), which increase the risk of embolism [1,2,5] and are associated with poor clinical outcomes in stroke patients [6]. Blood stasis in the LA/LAA is the main mechanism for developing LA/LAA thrombus and SEC in patients with AF [1,2]. Although shunt flow through the PFO may also affect LA/LAA hemodynamics [7], whether PFO influences LA/LAA thrombosis remains unclear. This study investigated the risk of LA/LAA thrombus or SEC in stroke patients with both AF and PFO.
This single-center retrospective cross-sectional study included patients with acute ischemic stroke who had nonvalvular AF and underwent transesophageal echocardiography (TEE) between 2011 and 2019 [4]. Patients who received LAA occlusion or PFO closure were excluded. The presence of PFO, LA/LAA thrombus, and SEC was determined using TEE. The measured echocardiographic parameters were LAA emptying velocity (LAAV), LA volume index, left ventricular ejection fraction, and ratio of early diastolic mitral inflow velocity to early diastolic mitral annular tissue velocity. This study was approved by the Institutional Review Board of Severance Hospital, Yonsei University Health System (no. 4-2022-1131), and the need for informed consent was waivered owing to its retrospective nature. Detailed information on the study population and echocardiographic evaluation are presented in the Supplementary Methods. Statistical analysis was performed using R version 4.0.4 (R Foundation for Statistical Computing, Vienna, Austria) and SAS version 9.4 (SAS Institute, Cary, NC, USA). Multivariable logistic regression analyses were performed to compare the frequencies of LA/LAA thrombus or SEC between patients with and without PFO. Mediation analysis was performed to evaluate echocardiographic parameters for explaining the relationship between PFO and LA/LAA thrombus or SEC [8].
Of the 1,469 stroke patients with AF, 696 with nonvalvular AF who underwent both TEE and TTE were included (Supplementary Figure 1) (median age=73 years, 59.2% male). Among them, 145 (20.8%) had PFO. LA/LAA thrombus or SEC was observed in 331 (47.6%) patients (thrombus in 82 [11.8%] and SEC in 321 [46.1%]).
LA/LAA thrombus or SEC was less frequent in patients with PFO than in those without (37.2% vs. 50.3%, P=0.007) (Table 1). In multivariable backward regression analysis, PFO was independently associated with a lower prevalence of LA/LAA thrombus or SEC (adjusted odds ratio [OR] 0.65, 95% confidence interval [CI] 0.44-0.96, P=0.028) (Table 2 and Supplementary Table 1). Additionally, PFO with high-risk features (a large shunt or atrial septal aneurysm) showed a stronger association (OR 0.39, 95% CI 0.16-0.94, P=0.037) (Table 2). LAAV was significantly higher in patients with PFO than in those without (35.0 [21.8-53.0] cm/s vs. 27.6 [18.3-46.5] cm/s, P=0.005) (Table 1).
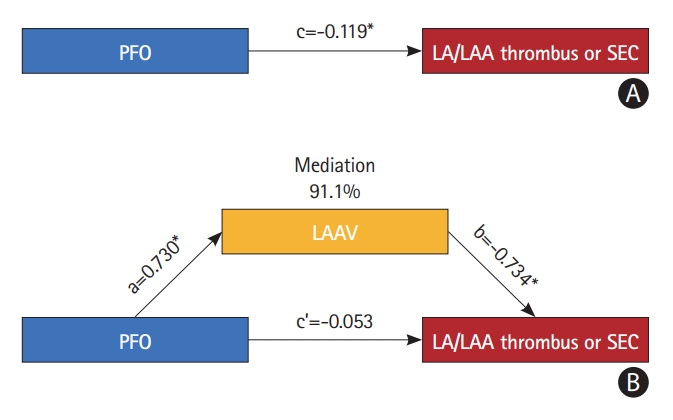
In the mediation analysis of echocardiographic parameters, LAAV was the only significant mediator for the effect of PFO on LA/LAA thrombus or SEC (91.1% mediation, P=0.031) (Figure 1 and Supplementary Table 2). The mediating effect was stronger in PFO patients with high-risk features (95.5% mediation, P=0.001) (Supplementary Table 3).
This study showed that PFO was associated with a lower prevalence of LA/LAA thrombus or SEC in stroke patients with nonvalvular AF, with the relationship likely to be mediated by higher LAAV.
In this study, LA/LAA thrombus or SEC was less frequent in patients with PFO than in those without. This result is in line with those of a previous study, which showed that LA/LAA thrombus or SEC was less frequent in patients with severe mitral stenosis and a coexisting PFO [9]. Although the cause-effect relationship remains uncertain, these findings suggest that PFO has a beneficial role in reducing LA/LAA thrombosis in patients with heightened thrombotic conditions. Stroke patients with determined etiologies, including AF, had a lower risk of recurrent stroke when they had a PFO [4]. It was speculated that PFO might be the actual etiology of stroke in some patients; therefore, the generally low-recurrence risk in PFO-associated stroke might be related to the decreased risk of stroke recurrence in such patients [4]. However, other factors may also be responsible for this low stroke risk. In AF, the presence of LA/LAA thrombus or SEC is an indicator of increased stroke risk [1,2]. Our findings suggest that coexisting PFO in patients with AF may reduce the risk of thromboembolism.
We also found that LAAV was significantly higher in patients with PFO than in those without. LAAV is a quantitative parameter for estimating thromboembolic risk, and a low LAAV has been associated with a higher risk of LA/LAA thrombus or SEC and thromboembolism [1,2]. Our findings suggest that intermittent shunt flow through the PFO may affect the flow dynamics in the LA/LAA, which was exhibited as a higher LAAV. These flow changes may act favorably to reduce blood stasis within the LA/LAA in patients with AF.
In this study, the decreased risk of LA/LAA thrombus or SEC in patients with PFO was almost exclusively explained by the increased LAAV. The mediating effect was stronger in PFO patients with high-risk features. Atrial remodeling and blood stasis are the key mechanisms of thrombosis in AF [1,2]. Considering the crucial role of slow flow in LA/LAA in thrombosis [1,2] and similar other demographic and clinical factors between patients with and without PFO, PFO-related changes in the LAAV may have played a major role in lowering the risk of thrombosis in this study population.
Ischemic stroke may recur even after PFO closure, and AF is a known potential procedure-related complication after PFO closure [7,10]. Our findings suggest that measuring LAAV may be necessary in patients undergoing PFO closure because the procedure may further decrease LAAV in patients with low LAAV, thereby may increasing the risk of LA thrombosis and ischemic stroke.
This study had several limitations. TEE could not be performed in nearly half of the stroke patients because of the requirement for patient cooperation. Consequently, this study included patients with milder strokes (Supplementary Table 4). The generalizability of the findings of this study may be limited because they were based on data from a single university hospital with a single ethnicity.
In conclusion, coexisting PFO decreased the risk of LA/LAA thrombus or SEC in stroke patients with AF, mainly by reducing blood stasis.