Stroke in young adults has a special significance in developing countries, as it affects the most economically productive group of the society. We identified the risk factors and etiologies of young patients who suffered ischemic strokes and were admitted to a tertiary referral hospital in North India.
Methods
A retrospective review of case records from patients with ischemic stroke in the age range of 18-45 years was conducted from 2005 to 2010. Data regarding patients' clinical profiles, medical histories, diagnostic test results, and modified Rankin Scale scores at hospital discharge were examined. Stroke subtyping was conducted in accordance with the Trial of Org 10172 in Acute Stroke Treatment (TOAST) criteria.
Results
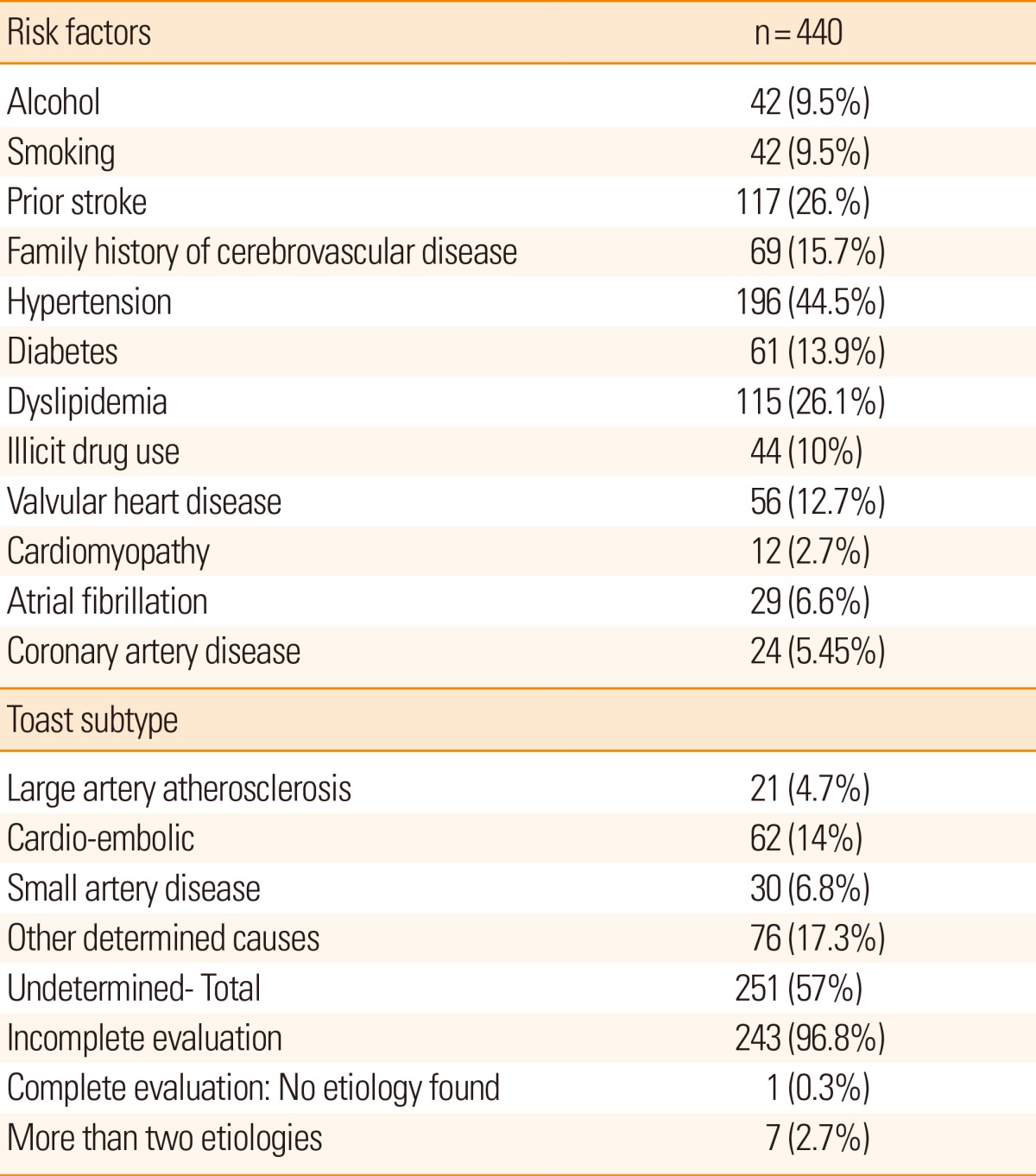
Of the 2,634 patients admitted for ischemic stroke, 440 (16.7%) were in the 18-45 year age range and the majority (83.4%) were male. The most common risk factors were hypertension (34.4%) and dyslipidemia (26.5%). The most common subtype of stroke was undetermined (57%), followed by other determined causes (17.3%). Among the category of undetermined etiology, incomplete evaluation was the most common. Most of the patients demonstrated good functional outcomes.
Conclusions
Young adults account for 16.7% of all stroke patients in North India. Risk factors are relatively prevalent, and a high proportion of the patients are categorized under undetermined and other determined causes. The results highlight the needs for aggressive management of traditional risk factors and extensive patient work-ups to identify stroke etiology in India.
Young adultIschemic strokeIndiaTOAST classification
Introduction
Ischemic strokes in young adults can have a significant impact on the affected individuals, their families, and societies in general, as the patients are affected in the economically productive period of their lives. Almost two thirds of the global burden of stroke is borne by those in developing countries.1 Young adults account for approximately 10%-30% of all stroke patients in India, as opposed to 3%-8.5% in Western countries.2,3,4 The etiologies of ischemic strokes in young adults are different and more diverse as compared to those observed in the elderly. Furthermore, etiological subtyping also varies according to geographical distribution. It is important to identify the causative factors in young stroke patients in order to prevent recurrences appropriately. Despite its substantial societal impact, there remains a paucity of literature regarding the etiological subtyping and risk factors for ischemic stroke in young Indian patients. The current study was conducted to identify ischemic stroke risk factors and etiological subtypes according to the Trial of Org 10172 in Acute Stroke Treatment (TOAST) criteria in young Indian patients.5
Methods
We conducted a retrospective chart review of patients who suffered an ischemic stroke from January 2005 to December 2010 and were admitted to a tertiary care hospital in North India. Ischemic stroke was defined as a sudden focal neurologic deficit with imaging-confirmed cerebral infarction. We excluded cases of intracranial hemorrhage, subarachnoid hemorrhage, and cerebral venous thrombosis.
From the total population of ischemic stroke patients, patients who had suffered an ischemic stroke and were in the age range of 18-45 years were enrolled. As a matter of protocol, all stroke patients admitted to the neurology wards underwent routine hematological and biochemistry tests (complete blood count, prothrombin time, activated partial thromboplastin time reactive protein, serum creatinine, blood glucose and lipid profile), chest X-rays, electrocardiography, and brain imaging including computed tomography (CT) and/or magnetic resonance imaging (MRI) at admission. Additionally, a majority of patients underwent vascular imaging studies such as MR angiography or CT angiography. Transthoracic echocardiography and Holter monitoring were performed in selected patients. More specific diagnostic testing (e.g. vasculitis profile) was performed when deemed necessary by the treating neurologist.
Patient case records were reviewed by a neurologist (AKP) and data regarding each patient's demographic profile, clinical presentation, medical history (emphasis on risk factors), results of vascular imaging, biochemical profile and other diagnostic tests, in-hospital treatment, and the modified Rankin Scale (mRS) score at hospital discharge were recorded in a structured proforma. Stroke subtyping was based on the information available at discharge and according to the TOAST criteria. Diabetes mellitus, hypertension, smoking, dyslipidemia, previous stroke or transient ischemic attack, migraine, atrial fibrillation, coronary artery disease, alcohol consumption, drug abuse, and family history of stroke among first and second-degree relatives were considered as risk factors. Etiological classification was analyzed by dividing the cohort into 2 groups according to age (18-35 years and 36-45 years) and by gender.
The recorded data were statistically analyzed for the percentage and mean and standard deviation of all variables. SPSS version 16.0 for windows was used for all statistical analyses. The χ2, Fisher's exact, and t tests were used as appropriate. P<0.05 was considered as statistically significant.
Results
Of 2,634 ischemic stroke patients admitted to our institute from January 2005 to December 2010, 440 patients were in the range of 18-45 years. The male-to-female ratio was 5:1, and the mean patient age was 38.9±7.1 years. Identified risk factors for ischemic stroke were hypertension (44.5%), dyslipidemia (26.1%), prior stroke or transient ischemic attack (TIA; 26%), family history of stroke (15.7%), and diabetes (13.9%) (Table 1). All patients underwent CT scans and 38.4% underwent MR angiography. Additionally, a carotid artery duplex scan was conducted in 85.7% of the patients. Holter monitoring was performed in 63% of patients, transthoracic echocardiography in 96.3%, and transesophageal echocardiography in 2.3%. A detailed work-up for coagulation disorders was conducted in 32% of the patients.
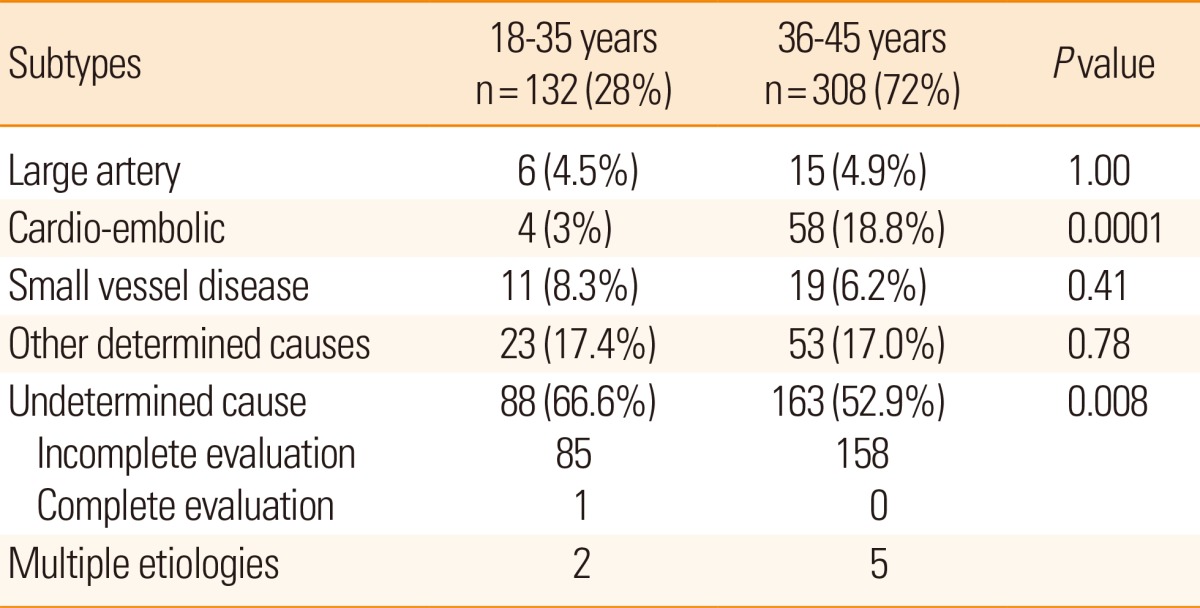
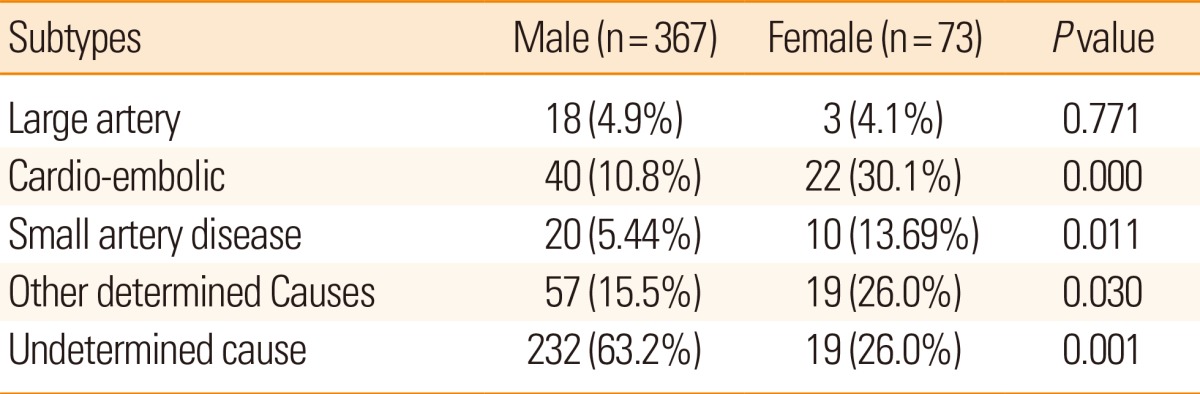
The anterior circulation was the most commonly involved vascular territory (74.2%), followed by the posterior circulation (21.1%), and strokes involving both territories (4.7%). The most common TOAST subtype was undetermined (57%), followed by other determined cause (ODC; 17.3%), and cardioembolism (14%) (Table 1). The etiological classification was also analyzed by dividing the cohort into 2 groups according to age (18-35 years and 36-45 years). The 36-45 year age group had a significantly higher percentage of patients with cardioembolic stroke (Table 2). When data were analyzed according to gender, the mean ages of male and females patients were 39.5±7.1 and 36.0±6.7 years, respectively (P=0.730). Women were more likely than men to have cardioembolism, small artery disease, and ODC (Tables 3, 4).
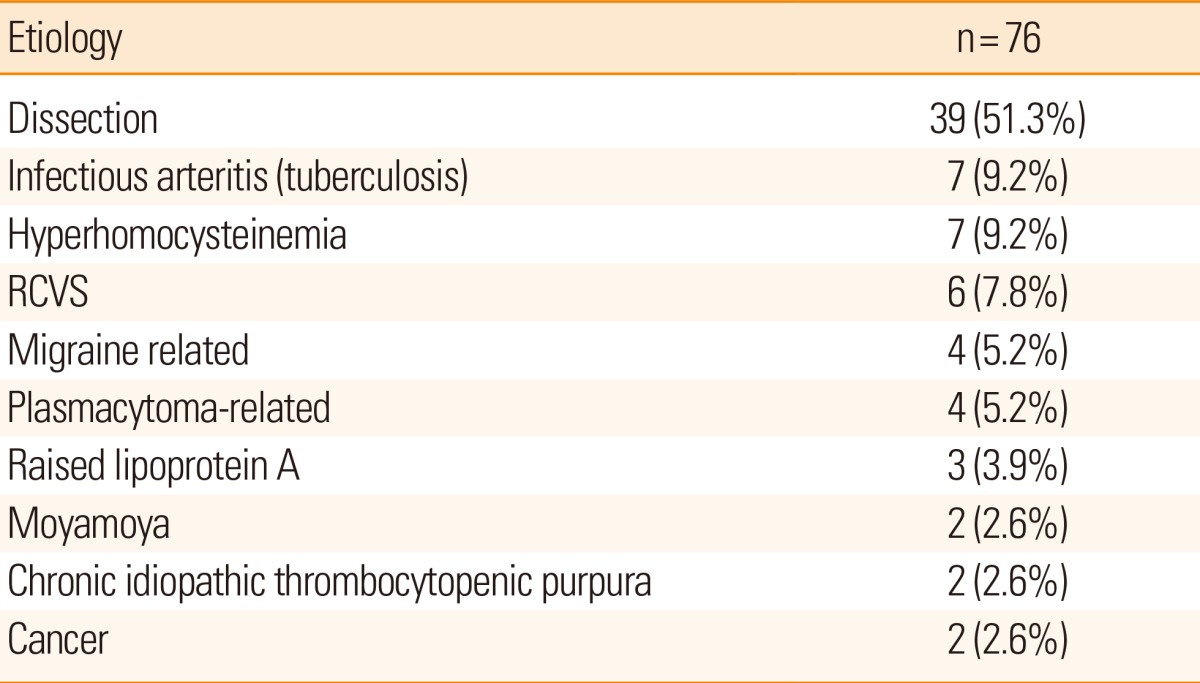
There were 76 patients who had ODC as an etiological subtype. The most common etiology in this group was dissection (Table 5). Among 39 cases of dissection, there were 37 patients with internal carotid artery dissection and 2 patients with vertebral artery dissection. The most common cause of cardioembolic stroke was valvular heart disease associated with rheumatic heart disease (44 patients, 70.1%). Cardiomyopathy was found in 4 (6%) patients, atrial fibrillation in 4 (6%), and others (i.e. infective endocarditis in 4 and myocardial infarction in 6) in 16.1%.
Regarding treatment, thrombolysis was performed in 3.9% of patients. Most (84%) of the patients were on an anti-platelet treatment with a majority (65.4%) receiving aspirin alone. Almost 88% of patients with a prior history of stroke and TIA had not taken any medications for the secondary prevention of stroke. At the time of hospital discharge, 392 (89%) patients had mRS scores in the range of 0-2, and 37 (8.4%) patients hand mRS scores of 3 or 4. Death was reported in 11 (2.5%) patients.
Discussion
By 2050, it is anticipated that 80% of stroke patients will be from the developing regions of the world.6 Additionally, there is growing evidence for an increasing trend in the incidence of stroke in young adults.7 Accurate classification of ischemic stroke is critical for guiding treatment decisions and determining the prognosis of individual patients. However, few studies have focused on the etiology and risk factors for ischemic stroke in young adults in India.8,9,10 The current study is the largest one focusing young stroke patients in India.
In comparison to studies conducted in Western countries, a higher male predominance was observed in the current study.11 The percentage was even higher than that reported from earlier studies from India.8,9 Because our institute is a referral center, patients are referred from all over the country. The male predominance noted in the current study may at least in part have been attributable to a sociocultural bias in India that manifests as males being more likely to seek treatment at referral centers than females. Similar to the previously published results,12,13 the current study identified a relatively high frequency of modifiable risk factors for ischemic stroke. Of these, hypertension and dyslipidemia were the most common. A significant number of patients had a history of prior stroke and TIA, and almost 88% of them were not taking any medications for the secondary prevention of stroke. This observation emphasizes the need for aggressive primary and secondary prevention targeting the traditional modifiable risk factors for young Indian subjects.
The most common stroke subtype in the current study was undetermined cause, and was observed at a higher rate than that reported in previous studies of ischemic stroke in young adults (24%-36%).12,14,15,16,17 The most frequent reason for categorizing these patients as having an undetermined etiology was an incomplete evaluation. Most of the patients did not have insurance and were therefore unable to afford the costs of radiological and biochemical diagnostic tests. The second most common etiology in the current study was stroke due to ODC. This result was comparable to the results of previous studies from Western countries.18,19,20
In a case controlled study of 214 first-occurrence ischemic strokes in young adults from South India, Lipska et al.9 reported that cardioembolic stroke (25.2%) was the most common stroke subtype, followed by large artery atherosclerosis (12.6%). They reported that 11.2% of patients had ODC. In another retrospective study of 177 young adult ischemic stroke patients from South India, the most common etiologic subtype was atherothrombotic stroke (24%), followed by cardioembolic stroke (17%).8 In contrast to the results of the current study, the aforementioned studies reported a low proportion of patients with ODC. This difference may be attributable to the non-availability of newer imaging techniques and diagnostic facilities in the previous studies, which could have resulted in an underreporting of ODC. In our study, the most common etiology under the category of ODC was cerebral artery dissections, which accounted for 51.3% of cases. The prevalence of cerebral artery dissection in young stroke patients has been reported to be in the range of 10%-20%.21 Similarly, 8.8% of patients in the current study were found to have dissections. Therefore, careful evaluation for cerebral artery dissection is pertinent in all young ischemic stroke patients. Detailed vascular imaging would also further increase the detection rates of other rare causes of stroke in young adults, such as Moyamoya disease and other vasculopathies.
The most common cause of cardioembolic stroke in the current study was valvular heart disease, with the majority having rheumatic heart disease (RHD). The incidence of cardioembolic stroke in young adults ranges from 14% to 47%.11,22,23,24 In the current study, cardioembolic stroke accounted for 14% of patients. Previous studies from India have reported RHD and prosthetic valves contributing to almost two thirds of all cardioembolic strokes in young adults.8,9 This highlights the need to develop preventive strategies targeting patients with RHD in order to ensure proper anticoagulation and medical follow-up for the disease. This is in contrast to the results of studies from developed countries where etiologies such as patent foramen ovale (PFO) or atrial septal defects (ASD) were more common than valvular heart disease as a cause of stroke.11,26 Another reason for underestimation of PFO/ASD could be the very low rate of transesophageal echocardiography performance (2.3%) in the current study. We found that a significantly higher percentage of the cardioembolic subtype was found in women, which is consistent with previous studies that reported a higher prevalence rate of RHD in women.27,28
In the current study, only 6.8% of patients were categorized as having small-vessel disease. TOAST defines small-vessel disease only if the subcortical lesions are smaller than 15 mm and large artery atherosclerosis only if there is stenosis (>50%) in the corresponding artery.5 Therefore, subcortical infarction of >15 mm in size and infarctions with vulnerable plaque with stenosis <50% should be classified as stroke of undetermined etiology. Thus, we may need a newer subtype classification in order to clarify these cases more accurately.29 The proportion of young patients with large artery atherosclerosis has traditionally been low in studies from Western countries.30,31 Despite the high prevalence of the traditional risk factors for stroke in our cohort, only 4.7% of patients were found to have large artery disease. This could be due to the fact that only 38.4% of our patients underwent intracranial vessel imaging.
In a prospective study of 198 young ischemic stroke patients, Nedeltchev and colleagues reported that 68% of patients achieved an mRS score of 0-1, 26% had an mRS score of 2-5, and 3% had died within 3 months.14 Putaala et al. found a functionally independent outcome (mRS score=0-2) in 80% of patients in a prospective study of 968 patients.31 In line with these results, good functional outcomes at discharge (mRS range=0-2) were observed in 89% of patients in our cohort. These results suggest relatively good functional outcomes in young stroke patients both in western countries and in India.
The current study has several limitations, the first being the retrospective design. Because patients were recruited over a long period of time, differences in the work-up strategy with regard to advanced imaging and other diagnostic technologies may have been introduced. Furthermore, not all patients underwent detailed studies such as tests for coagulation abnormalities, vascular imaging, and transesophageal echocardiography. Lastly, this is a hospital-based study and the results may not be generalizable to the general population. Despite these limitations, the current study is the largest one focusing on the etiologies and risk factors for ischemic stroke in young adults in India. Our study highlights the need for aggressive management of traditional risk factors in young adults and also the need for extensive work-up in every patient in order to find correct etiologies.
The authors have no financial conflicts of interest.
BonitaRMendisSTruelsenTBogousslavskyJTooleJYatsuFThe global stroke initiativeLancet Neurol2004339139315207791KaulSBandaruVCSuvarnaABodduDBStroke burden and risk factors in developing countries with special reference to IndiaJ Indian Med Assoc200910735837019886374NagarajaDGururajGGirishNPandaSRoyAKSarmaGRFeasibility study of stroke surveillance: data from Bangalore, IndiaIndian J Med Res200913039640319942742NenciniPInzitariDBaruffiMCFratiglioniLGagliardiRBenvenutiLIncidence of stroke in young adults in Florence, ItalyStroke1988199779983400108AdamsHPJrBendixenBHKappelleLJBillerJLoveBBGordonDLClassification of subtype of acute ischemic stroke: definitions for use in a multicenter clinical trialStroke19932435417678184FeiginVLStroke epidemiology in the developing worldLancet20053652160216115978910GeorgeMGTongXKuklinaEVKuklinaEVLabartheDRTrends in stroke hospitalizations and associated risk factors among children and young adults, 1995-2008Ann Neurol20117071372121898534NayakSDNairMRadhakrishnanKSarmaPSIschemic stroke in the young adult: clinical features, risk factors and outcomeNatl Med J India1997101071129230597LipskaKSylajaPNSarmaPSThankappanKRKuttyVRVasanRSRisk factors for acute ischaemic stroke in young adults in South IndiaJ Neurol Neurosurg Psychiatry20077895996317220290MehndirattaMMAgarwalPSenKSharmaBStroke in young adults: a study from a university hospital in north IndiaMed Sci Monit200410CR535CR54115328488JiRSchwammLHPervezMASinghalABIschemic stroke and transient ischemic attack in young adults: risk factors, diagnostic yield, neuroimaging, and thrombolysisJAMA Neurol201370515723108720YouRXMcNeilJJO'MalleyHMDavisSMThriftAGDonnanGARisk factors for stroke due to cerebral infarction in young adultsStroke199728191319189341695RohrJKittnerSFeeserBHebelJRWhyteMGWeinsteinATraditional risk factors and ischemic stroke in young adults: the Baltimore-Washington Cooperative Young Stroke StudyArch Neurol1996536036078929167NedeltchevKder MaurTAGeorgiadisDArnoldMCasoVMattleHPIschemic stroke in young adults: predictors of outcome and recurrenceJ Neurol Neurosurg Psychiatry20057619119515654030VaronaJFGuerraJMBermejoFMolinaJAGomez de la CamaraACauses of ischemic stroke in young adults, and evolution of the etiological diagnosis over the long termEur Neurol20075721221817268202KittnerSJSternBJWozniakMBuchholzDWEarleyCJFeeserBRCerebral infarction in young adults: the Baltimore-Washington Cooperative Young Stroke StudyNeurology1998508908949566368RasuraMSpalloniAFerrariMDe CastroSPatellaRLisiFA case series of young stroke in RomeEur J Neurol20061314615216490045CerratoPGrassoMImperialeDPrianoLBaimaCGiraudoMStroke in young patients: etiopathogenesis and risk factors in different age classesCerebrovasc Dis20041815415915256790GhandehariKMoudZIIncidence and etiology of ischemic stroke in Persian young adultsActa Neurol Scand200611312112416411973GroppoEDe GennaroRGranieriGFazioPCesnikEGranieriEIncidence and prognosis of stroke in young adults: a population-based study in Ferrara, ItalyNeurol Sci201233535821695657SchievinkWISpontaneous dissection of the carotid and vertebral arteriesN Engl J Med200134489890611259724ChanMTNadareishviliZGNorrisJWDiagnostic strategies in young patients with ischemic stroke in CanadaCan J Neurol Sci20002712012410830344FerroJMCrespoMPrognosis after transient ischemic attack and ischemic stroke in young adultsStroke199425161116168042212Yesilot BarlasNPutaalaJWaje-AndreassenUVassilopoulouSNardiKOdierCEtiology of first-ever ischaemic stroke in European young adults: the 15 cities young stroke studyEur J Neurol2013201431143923837733Siqueira NetoJISantosACCabete FabioSRSakamotoACCerebral infarction in patients aged 15 to 40 yearsStroke199627201620198898808PutaalaJMetsoAJKonkolaNKraemerYHaapaniemiEKasteMAnalysis of 1,008 consecutive patients aged 15 to 49 with first-ever ischemic stroke: the Helsinki young stroke registryStroke2009401195120319246709KimBJKimJSIschemic stroke subtype classification: an Asian view pointJ Stroke20141681724741560BogousslavskyJPierrePIschemic stroke in patients under age 45Neurol Clin1992101131241556998LeysDBanduLHénonHLucasCMounier-VehierFRondepierrePClinical outcome in 287 consecutive young adults (15 to 45 years) with ischemic strokeNeurology200259263312105303Siqueira NetoJISantosACFabioSRSakamotoACCerebral infarction in patients aged 15 to 40 yearsStroke199627201620198898808PutaalaJStrbianDMustanojaSHaapaniemiEKasteMTatlisumakTFunctional outcome in young adult ischemic stroke: impact of lipoproteinsActa Neurol Scand2013127616922616937